| Impotence, Erectile Dysfunction, ED (What every Adult needs to know) |
| ANDROLOGY : The Science of Dysfunctions of the Male Reproductive System |

 | |
| Sex is Not a Four-Letter Word | |
| Publisher: Rupa & Co., India | |
| A sex edutainment book by Dr. Sudhakar Krishnamurti... |
|
| Check with a good bookstore near you! | |
| Buy Online at | |
| • | Rediff Books |
| • | Google.com |
| • | Amazon.com |
| • | NDTV Fabmall |
| • | Linux Bazar |
| A G A S S I 'Ageing, Gender, Andrology, & Sexual (Sciences), Society of India'
|
|
 Though ejaculation often occurs normally and is an intensely pleasurable sensation for most men, it is an extremely complex phenomenon that is regulated by many different systems. Hence, things often can, and do go wrong. |
 Impotence often comes without warning and can strike even the most virile stud like a bolt of lightning. How much of a risk do you face ? |
The vacuum device is an external, non-invasive treatment option for impotence.
This device is available for purchase through this site.
Please Contact Us
More Information on non-invasive treatment options. More Details
 Before the advent of andrology, it was both thought and taught that impotence was psychological in origin. Epoch-making andrologic research in the past decade has shattered this myth and today it is known that in 80-90% of such cases, there is a physical (organic) cause rather than a purely psychological (functional) one. |
 We've all heard of the barren wife. But what of barren husbands ? Can male infertility be cured ? The wife visits her gynecologist...so who is the husband supposed to consult ? find out in THE MALE FACTOR IN INFERTILITY |
|
Even today,
These two factors explain why most cases of impotence do not come to light and why the few that do are grossly mismanaged. It is not surprising, therefore, that the general impression is that impotence is something largely incurable. This is unfortunate because not only are most cases of impotence NOT psychological in origin but most are EMINENTLY CURABLE as well. Impotence, or erectile dysfunction (ED, E.D.), as andrologists prefer to call it, has always been and continues to remain an extremely common disorder. It is said to afflict as much as 10 percent of the male population. Above the age of 40, nearly 52 % of men are affected. Despite this staggering incidence, few cases come to light. Contrary to popular belief, impotence is almost never an 'all or none' phenomenon. Most laymen (and several doctors) believe that a man can either have an erection of very good quality or none at all. Nothing can be farther from the truth. Most men with erectile dysfunction have normal desire and can obtain an erection, only the erection is not hard enough or doesn't last long enough, Hence the term erectile dysfunction (which suggests partial loss) is preferred to impotence (which suggests a total loss). Not many are aware that in most cases organic rather than psychological causes are responsible.
However, the trend is slowly but definitely changing. This is largely due to tremendous advances in andrological research over the past few years which have conclusively established that in as many as 80-90 percent of cases of chronic impotence, the cause is not in the mind but in the body. These causes can be identified using modern andrological investigative modalities, quantified and often successfully treated using totally non-psychological methods. In an era where so many advances have been made in nearly all other branches of medicine, it is surprising that male reproductive system research has remained so woefully neglected and backward. For instance, the branch of obstetrics and gynecology (the female analogue of andrology) which deals with disorders of the female reproductive system has been with us for several decades now and is a well recognised specialty. In fact, so advanced is the understanding of the subject that today, in most countries, gynecologists restrict themselves to sub-specialty areas within their subject such as gynecological oncology, high-risk pregnancies, female infertility etc. because it is so difficult to keep pace with all the developments in the subject.
It may be of interest to our readers to deliberate in passing the reasons for this delayed understanding of the subject.
Two factors are predominant. The first of these is male chauvinism. Throughout human history, most of our societies have been patriarchal and male-dominated. Men's egos would not let them admit that there could be something wrong with their 'jewels of manhood'. Ironically, it is these very men who researched the female reproductive system and helped develop the branch of gynecology and obstetrics. But they refused to look into themselves. The second reason is a misinterpretation of the teachings of Sigmund Freud. This led to the erroneous conclusion that most male sexual problems had their roots in the mind. Whereas most branches of medicine have taken their roots from biology - the study beginning with an understanding of the anatomy(structure) and physiology(function) of that part, and proceeding to then figure out what happens when anatomy or physiology goes wrong thus causing disease (pathology), the male reproductive system alone took its roots from psychology rather than biology, thus causing tremendous damage. This explains why most people know that it takes a complex concatenation of neuromuscular phenomena to lift a finger but fail to realize that equally complex phenomena are needed to lift the penis!! Most think that all that is needed for the latter event to occur is a naughty thought. What then causes impotence(ED) ? Although ED (impotence) can afflict anyone from 13 to 90 and is associated with a wide variety of clinical conditions and disease states (see box above), the basic mechanisms causing impotence are only a few. All of these can be accurately identified using modern andrological investigative techniques.
Impotence can be of several types :
Arteriogenic impotence resulting from injuries is very common but often unsuspected because of ignorance of the causative conditions. Many such patients are to be found in orthopedic and urology wards. The impotence is often discovered much later, after the more obvious wounds and fractures have healed. Ironically, it is most often discovered by the patient himself and not by the doctor.
Venogenic impotence is extremely common. It is said to account for as much as 30-70 percent of all impotence. Some men have venogenic impotence from birth (primary). Such men have never had a rigid erection all their lives. Others develop venogenic impotence suddenly after years of normal sexuality (secondary).
Many things can go wrong with the nerve supply to the penis. Injuries to the back, especially if they involve the vertebral column and the spinal cord can cause impotence. So also can injury to other nerves supplying the penis such as occurs after pelvic or perineal trauma. A wide variety of operations performed for other conditions can cause incidental injury to the nerves of the penis and cause impotence. These include operations on the rectum, prostate, urethra, spine, retroperitoneum, urinary bladder etc.. Of course, disorders of the nervous system such as multiple sclerosis, myelitis, tumour etc. are wont to cause impotence if they involve the nerve supply to the penis. Another disease affecting the nerves to the penis is diabetes mellitus. Impotence is extremely common among diabetics. In fact, as many as 50 per cent of all diabetics are impotent. Impotence in diabetics is almost always organic in origin. Appropriate therapy for diabetes can never restore erectile function because the basic diabetic process can never be reversed. Only the blood sugar levels and the complications of diabetes are controlled. Modern andrology, however, can offer a cure to nearly all patients with diabetes-related impotence. This is another fact that is, unfortunately, not known to most people. Few diabetologists address erectile dysfunction (ED, impotence) in their patients.
Many drugs also cause neurogenic impotence by affecting the neurotransmitters at the nerve endings. Notable among these are anti-hypertensives (BP lowering) and psychotropics. The list is very large. Often, it is not known that the medicine (which is prescribed for some unrelated disease, such as duodenal ulcer) is the culprit.
Another group where mixed factors operate is where long standing impotence has led to secondary psychiatric disorders such as depression etc.. Here, the basic causative factor is organic but being unrecognised and untreated (or maltreated) it eventually takes its toll on the mind, often because the patient thinks or has been led to believe that the condition is incurable and that it's all in his mind.
Only then can treatment proceed in a scientific and systematic manner.
There are several treatment options for impotence. This is a very brief discussion on some of the options.
Effective oral medication has re-written the management of ED and is effective in nearly 70 - 75 % of cases. Several internet resources are available for more detailed information about these drugs and these will not be discussed in detail here.
Side effects, include petechiae (reddish, pinpoint-size dots) and ecchymoses (bruising). These conditions are not painful or serious and generally occur only during an initial learning period. Penile temperature may decrease 1-2 degrees during use. Vacuum devices are generally favoured by elderly patients with erectile dysfunction.
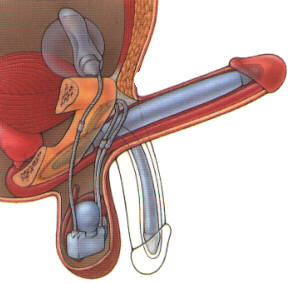
Erections obtained by injection usually last 30-60 minutes and may not subside when a man has an orgasm or ejaculates, and may interfere with the patient's social/business agenda. An overdose can cause a prolonged and painful erection that may require medical or surgical intervention. Frequent use may lead to the build-up of scar tissue in the penis, further complicating the process of erection.
|
|||||||||||||||||||||||||||||||||||||||||||||||
Home | News | Main Articles | Special Features | |||||||||||||||||||||||||||||||||||||||||||||||
 Not many people are aware that in most cases physical rather than psychological causes are responsible for impotence (ED), and that ED is usually eminently curable.
Not many people are aware that in most cases physical rather than psychological causes are responsible for impotence (ED), and that ED is usually eminently curable.